

Against decorative statistics
Against decorative statistics
And toward data minimalism

On the pernicious popularity of “decorative statistics.”
I’m not sure if this phrase is new, but it cleverly encapsulates an issue that’s frustrated me for years.
Long COVID statistics are one notable example of this. Last year, I attempted to sort out whether the extreme numbers being thrown around were justified by other data sources.
The absurd idea that medical errors are the third leading cause of death is another decorative statistic that I’ve fought back against here and here and here.
Long COVID and medical errors are both serious and common problems. This can weaken our resolve to push back against inaccurate analyses when appropriate.
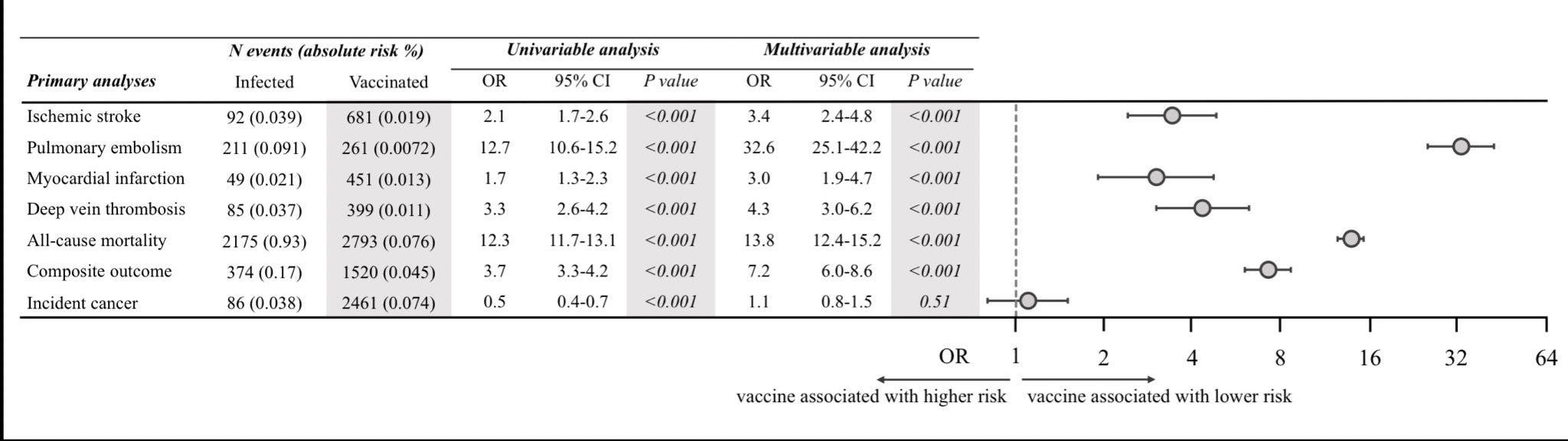
On the increased risk of heart attack, blood clot, and stroke from COVID compared to the vaccines, this time from a decent Danish study.
It’s easy to get distracted or overwhelmed by the deluge of observational COVID data. Let’s be clear: most studies have not used appropriate data sources or controls to truly understand the myriad potential post-infection health outcomes. Even good studies should be replicated given the analytic flexibility inherent in this process.
It’s nearly impossible now to separate out useful results from seriously flawed analyses. Scientists and journalists have shown little restraint in choosing which reports to highlight.
Nevertheless, the best studies we have show a real thromboembolic risk after COVID, likely attenuated by vaccination.
My article on “medium COVID,” an attempt to unify higher quality data into some understanding of how short- and medium-term risks from the virus are likely to differ from long-term outcomes.
My article on the now mainstream anti-vax campaign to falsely paint the COVID shots as having frequent cardiac risks.
On the continued vulnerability of our public health laboratory infrastructure.
My article from last summer on the regulatory failures of monkeypox (mpox) testing.
On using diagnostic stewardship to prevent medical errors.
Thanks for reading,
Ben